


Introduction:
Clinical outcomes of patients with Philadelphia chromosome positive (Ph+) B-ALL have been significantly improved with the addition of tyrosine kinase inhibitors (TKIs). The treatments with a TKI alone or a TKI with chemotherapy result in morphological complete response in nearly all patients with Ph+ B-ALL. However, persistence of measurable residual disease (MRD) and disease relapse remain major clinical problems (Ravandi et al. Blood 2019). Identification of predictive and prognostic biomarkers for Ph+ B-ALL is urgently needed.
Recurring genetic abnormalities such as deletions in IKZF1, CDKN2A/2B, PAX5, BTG1, and EBF1 have been identified in Ph+ B-ALL (Mullighan et al. Nature 2008). Among those, IKZF1 deletion has been associated with poor prognosis in Ph+ B-ALL patients treated with imatinib-based or dasatinib-based regimens. However, molecular determinants for clinical outcomes in ponatinib (potent TKI)-treated patients are not known. Here, we have systematically analyzed genetic alterations in adult Ph+ B-ALL patients uniformly treated in clinical trials with Hyper-CVAD plus dasatinib or Hyper-CVAD plus ponatinib regimens and investigated the molecular determinants for treatment outcomes and prognosis.
Methods:
We analyzed pretreatment bone marrow or peripheral blood specimens collected from adults with Ph+ B-ALL, who participated in clinical trials with either NCT00390793 (Hyper-CVAD plus dasatinib, N = 55) or NCT01424982 (Hyper-CVAD plus ponatinib, N = 50). Targeted capture DNA sequencing of 295 genes (N = 102) or whole exome sequencing (WES, N = 3) was performed. Genome-wide copy number analysis (CNA) was performed using either SNP microarray (N = 102) or WES (N = 3).
Results:
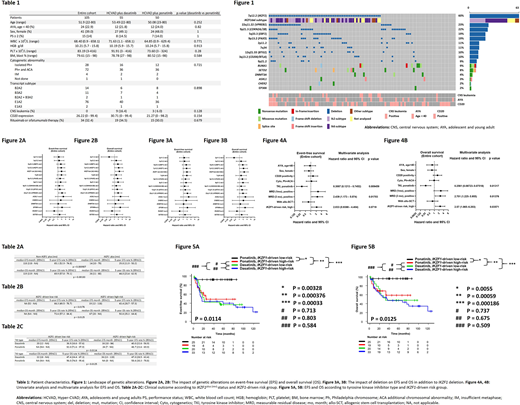
Baseline clinical characteristics of these patients are described in Table 1. The landscape of genetic alterations, which summarizes the CNAs and point mutations detected is shown in Figure1. The most frequently detected alterations were IKZF1 deletion. Among the 63 cases with IKZF1 deletion, we addressed detailed deletion site in 53 cases. Ik6 subtype, which is characterized by deletion of exon 4-7 (N = 28, 23 %) was most frequently detected followed by Ik2 subtype, which involves deletion of exon 2 (N = 20, 32 %).
Figure 2A and 2B show the impact of each genetic alteration on event-free survival (EFS) and overall survival (OS). Cases harboring Ik2 subtype deletion or Ik6 subtype deletion showed significantly worse EFS (hazard ratio [HR] = 1.91; p = 0.048) and OS (HR = 2.36; p = 0.019) than non-IKZF1 deletion cases or cases with IKZF1 deletion other than Ik2 or Ik6 subtype. We defined the IKZF1plus group as the group consisting of the cases with deletion of IKZF1 and other deletions. Then, we performed univariate analysis for cases with IKZF1 deletion in order to find the significant deletion partner of IKZF1 deletion in terms of prognosis (Figure 3A and 3B) and we defined IKZF1plus(rev) group as cases IKZF1 deletion with both CDKN2A/2B deletions and VPREB1 deletion or, or at least one of them. IKZF1plus(rev) group showed worse prognosis on EFS and OS than non-IKZF1plus(rev) group (Table 2A).
Combining the results of the impact of Ik subtype and IKZF1plus(rev) group on EFS and OS, we defined IKZF1-driven high-risk group as cases harboring either alteration of Ik2/Ik6 subtype or IKZF1plus(rev). IKZF1-driven high-risk group showed worse prognosis on EFS and OS than IKZF1-driven low-risk group (Table 2B).
Next, we performed univariate analysis and multivariate analysis combining baseline features, TKI type, and MRD status to assess their impact on outcome (Figure 4A and 4B). Multivariate analysis showed TKI type, MRD status at 3 months, and IKZF1-driven high-risk group were independent factors for OS. (Figure 4B).
Figures 5A and 5B show EFS and OS according to TKI type and IKZF1-driven risk. In patients treated with Hyper-CVAD plus ponatinib and categorized into IKZF1-driven low-risk group, the 5-year EFS and OS rates were 92.0% and 96.0%, respectively (Table 2C).
Discussion:
In this study, unlike with dasatinib-based therapy, we demonstrated that IKZF1-driven high-risk group was associated with worse EFS and OS than IKZF1-driven low-risk in the context of Hyper-CVAD plus ponatinib. Evaluation of the prognostic implication of Ph+ B-ALL using IKZF1-driven risk group at the time of the diagnosis may be useful to personalize treatment in order to improve the clinical outcome of Ph+ B-ALL in the era of ponatinib.
Kantarjian:Pfizer: Honoraria, Research Funding; Novartis: Honoraria, Research Funding; Adaptive biotechnologies: Honoraria; Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees; Sanofi: Research Funding; Amgen: Honoraria, Research Funding; Abbvie: Honoraria, Research Funding; Jazz: Research Funding; Immunogen: Research Funding; Ascentage: Research Funding; BMS: Research Funding; Daiichi-Sankyo: Honoraria, Research Funding; Janssen: Honoraria; Delta Fly: Honoraria; Oxford Biomedical: Honoraria; Aptitute Health: Honoraria; BioAscend: Honoraria. Short:Takeda Oncology: Consultancy, Honoraria, Research Funding; Amgen: Honoraria; Astellas: Research Funding; AstraZeneca: Consultancy. Jain:TG Therapeutics: Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Genentech: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Fate Therapeutics: Research Funding; Pharmacyclics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Adaptive Biotechnologies: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; AstraZeneca: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Precision Bioscienes: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; BMS: Research Funding; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Verastem: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Aprea Therapeutics: Research Funding; ADC Therapeutics: Research Funding; Incyte: Research Funding; Servier: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Cellectis: Research Funding; Pfizer: Research Funding; BeiGene: Honoraria, Membership on an entity's Board of Directors or advisory committees. Sasaki:Novartis: Consultancy, Research Funding; Daiichi Sankyo: Consultancy; Pfizer Japan: Consultancy; Otsuka: Honoraria. Ravandi:BMS: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria; Abbvie: Consultancy, Honoraria, Research Funding; Xencor: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy, Honoraria; Amgen: Consultancy, Honoraria, Research Funding; Astellas: Consultancy, Honoraria, Research Funding; Orsenix: Consultancy, Honoraria, Research Funding; Jazz Pharmaceuticals: Consultancy, Honoraria, Research Funding; Macrogenics: Research Funding. Konopleva:Ascentage: Research Funding; Calithera: Research Funding; Reata Pharmaceutical Inc.;: Patents & Royalties: patents and royalties with patent US 7,795,305 B2 on CDDO-compounds and combination therapies, licensed to Reata Pharmaceutical; Forty-Seven: Consultancy, Research Funding; Amgen: Consultancy; AstraZeneca: Research Funding; F. Hoffmann La-Roche: Consultancy, Research Funding; Agios: Research Funding; Cellectis: Research Funding; Kisoji: Consultancy; Sanofi: Research Funding; Ablynx: Research Funding; Rafael Pharmaceutical: Research Funding; Genentech: Consultancy, Research Funding; AbbVie: Consultancy, Research Funding; Stemline Therapeutics: Consultancy, Research Funding; Eli Lilly: Research Funding. Garcia-Manero:AbbVie: Honoraria, Research Funding; Onconova: Research Funding; Bristol-Myers Squibb: Consultancy, Research Funding; Amphivena Therapeutics: Research Funding; Acceleron Pharmaceuticals: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; H3 Biomedicine: Research Funding; Helsinn Therapeutics: Consultancy, Honoraria, Research Funding; Astex Pharmaceuticals: Consultancy, Honoraria, Research Funding; Jazz Pharmaceuticals: Consultancy; Novartis: Research Funding; Genentech: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Merck: Research Funding. Jabbour:BMS: Other: Advisory role, Research Funding; Amgen: Other: Advisory role, Research Funding; Genentech: Other: Advisory role, Research Funding; Pfizer: Other: Advisory role, Research Funding; AbbVie: Other: Advisory role, Research Funding; Adaptive Biotechnologies: Other: Advisory role, Research Funding; Takeda: Other: Advisory role, Research Funding.
This icon denotes a clinically relevant abstract

